Radiographic Projections
In evaluation of the arthritides, the two most important radiographic projections of the hands are:
- Posterior-Anterior (PA)
- Anterior-Posterior Oblique (“Ball-Catcher’s”)
- Other radiographic projections include:
- Lateral projection - used mainly in trauma and is of less importance in rheumatology
- PA Oblique
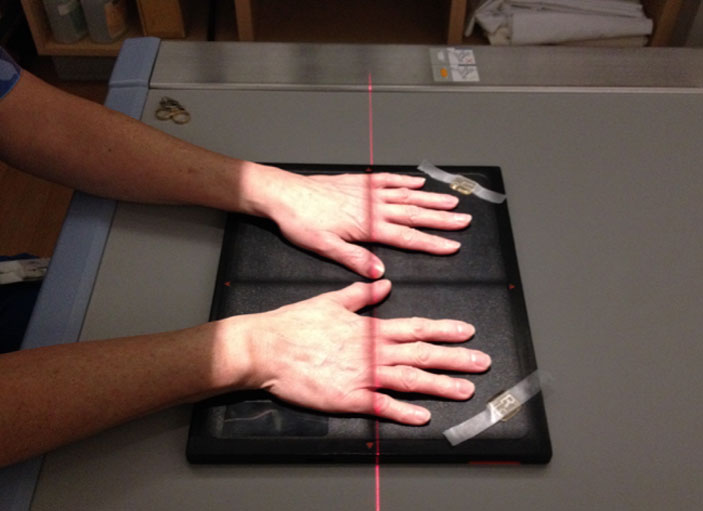
Posterior-Anterior Projection (PA)
- Radiograph is shot from above with palms of hands flat on cassette.
- Include entire hand and distal 2-3cm of the radius
- Centered to the third MCPJ (metacarpophalangeal joint)
- Excellent for assessment of joint spaces, bone density, soft tissue swelling and non-reducible subluxation/deformities.

Anterior-Posterior Oblique projection (“Ball-Catchers”)
- Hands are obliqued 45 degrees, AP projection and centred between the hands at the level of the MCPJs
- This projection is optimal for seeing early erosions at the MCP joints, especially at radial margins of 2nd to 5th MCPJs, pisotriquetral joint and the 3-5th carpo-metacarpal joints.


Wrist Radiographs
- The wrist may be imaged separately from the hand.
- Usually performed for localized pathology including fractures, infection, SLAC wrist etc.
- Views include:
- PA
- PA Internal Oblique
- PA External Oblique
- Lateral
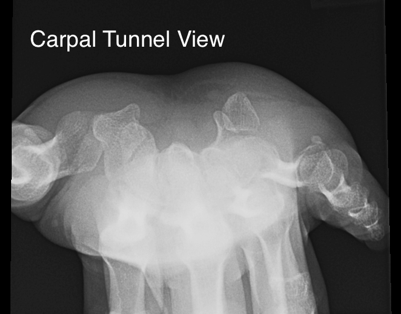
- Carpal Tunnel
- Scaphoid views
Wrist Radiographs

Wrist Radiographs




Tomosynthesis
- This is similar to conventional tomography. However in tomosynthesis only one sweep of the x-ray tube is made during which multiple exposures are taken which can be reconstructed to produce multiple images at different levels
- The x-ray tube follows a small rotation angle of <40°. The thickness of each slice can be changed depending on the anatomy of the structure being investigated.
- There has seen a resurgence of interest in tomosynthesis during the last decade with the availability of flat panel radiographic detectors that would allow low noise rapid image acquisition without geometric distortion.
- Recent research has demonstrated increased sensitivity and specificity for erosive disease in the hands and wrists .
- The radiation exposure is low, comparing 30 x1mm slices with 2 standard radiographs of the hands, the radiation dose is less than 3 times that of standard radiographs.
- Tomosynthesis will likely play a significant role in the future in the detection of erosive disease in rheumatology.
 info_outline
info_outline
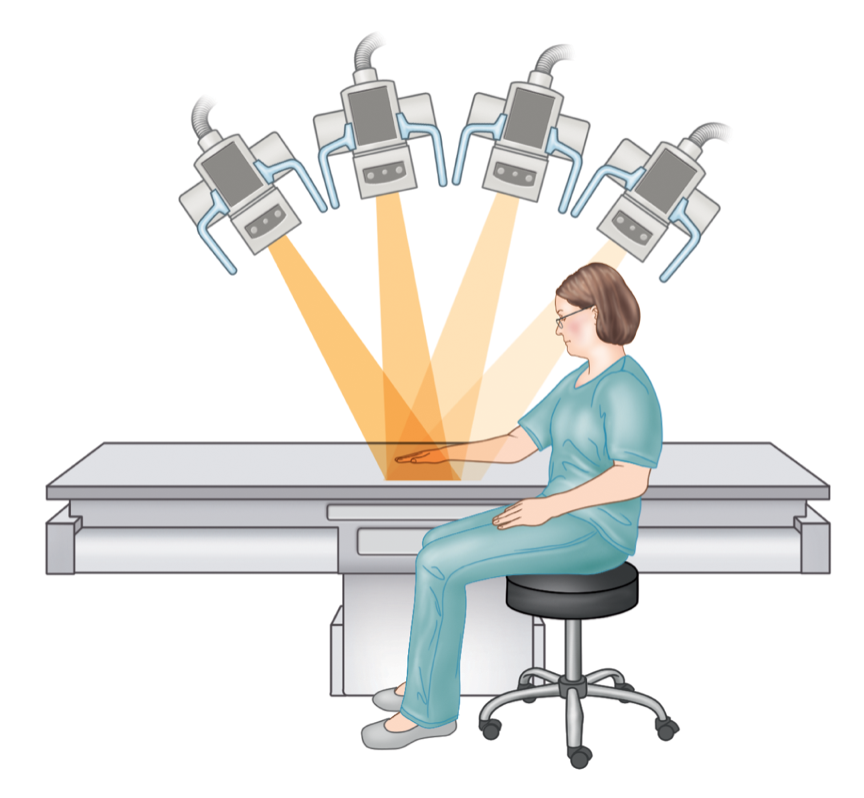
Illustration demonstrating the acquisition of a tomosynthesis series of the hand, note the arc of the x-ray tube as the images are acquired.
Illustration demonstrating the acquisition of a tomosynthesis series of the hand, note the arc of the x-ray tube as the images are acquired.
PA radiograph of the right hand demonstrates degenerative changes in this patient with CPPD arthropathy and rheumatoid arthritis. No erosive disease identified. Tomosynthesis series , b-g, demonstrate an erosion on the second metacarpal head (arrow) barely perceptible on PA radiograph, and marginal erosions at the base of the proximal phalanx (arrowheads on c) not seen on the PA radiograph (a).


Conventional Tomography
- This has gained a lower position on the imaging options with the advent of cross-sectional imaging techniques such as CT and MRI.
- The X-ray source and detector are moved in a set path during an exposure. Anatomy at a set depth remains in focus while structures at superficial and deeper levels are blurred.
- It is rarely used in the radiology department