Common Sites Involvement Of The Major Arthritides
Osteoarthritis (Primary)
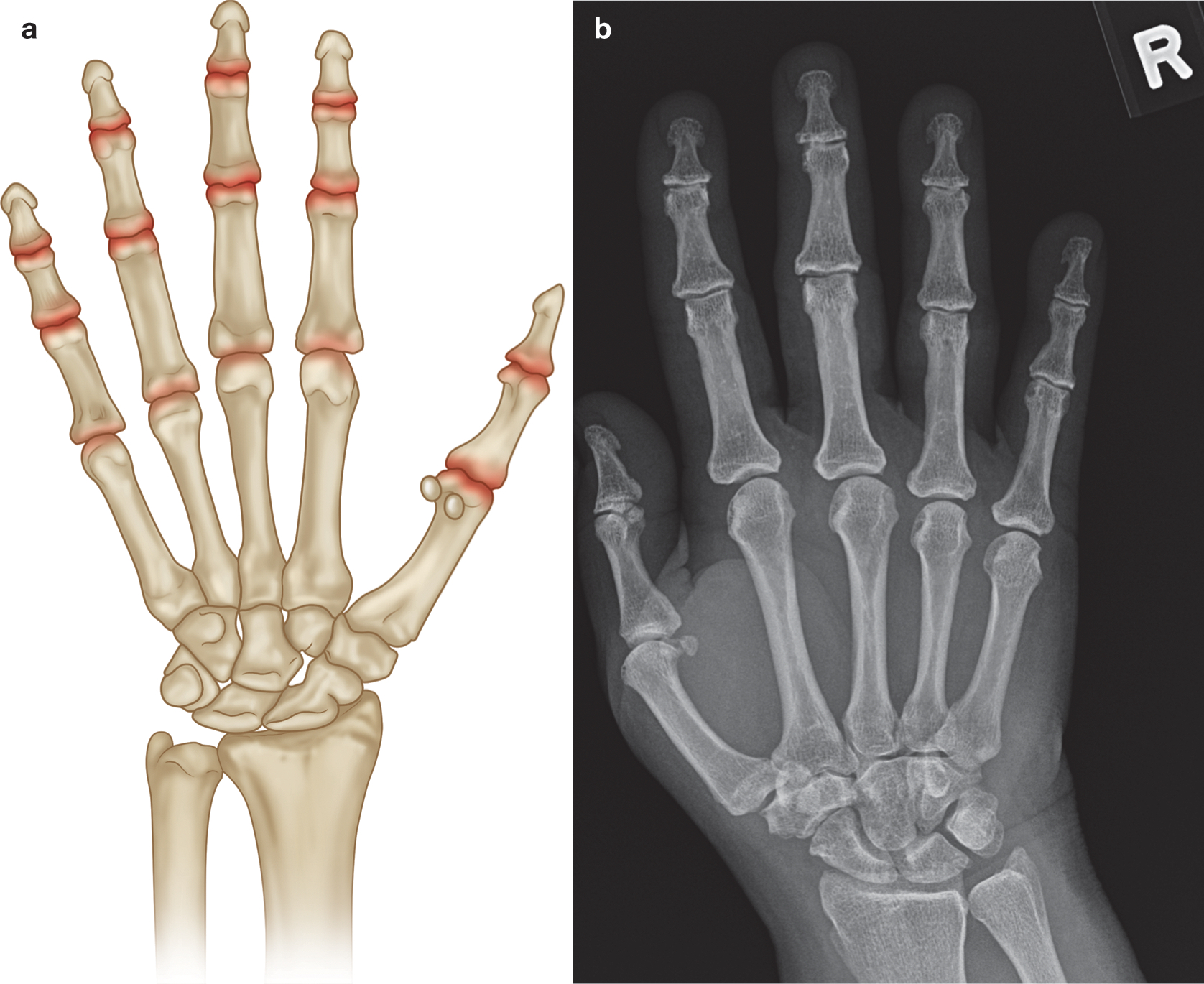
- Typical distribution of affected joints and the subsequent pattern recognition are key elements in helping the clinician arrive at a diagnosis.
- DIPJs, PIPJs, and the first CMCJ are classically associated with primary OA. If other joints of the hand are involved with OA, one should think of secondary causes to include crystal disease, RA, and trauma.
- The second and third MCPJs are an unusual site of primary OA and, if noted, should prompt one to think about CPPD and more importantly its associated etiologies such as hemochromatosis (which shouldn’t be missed).
Other Joints
- Symmetrical involvement of the PIP, MCP, and wrist joints (symmetry is a key feature in that both hands are involved rather than perfect symmetry).
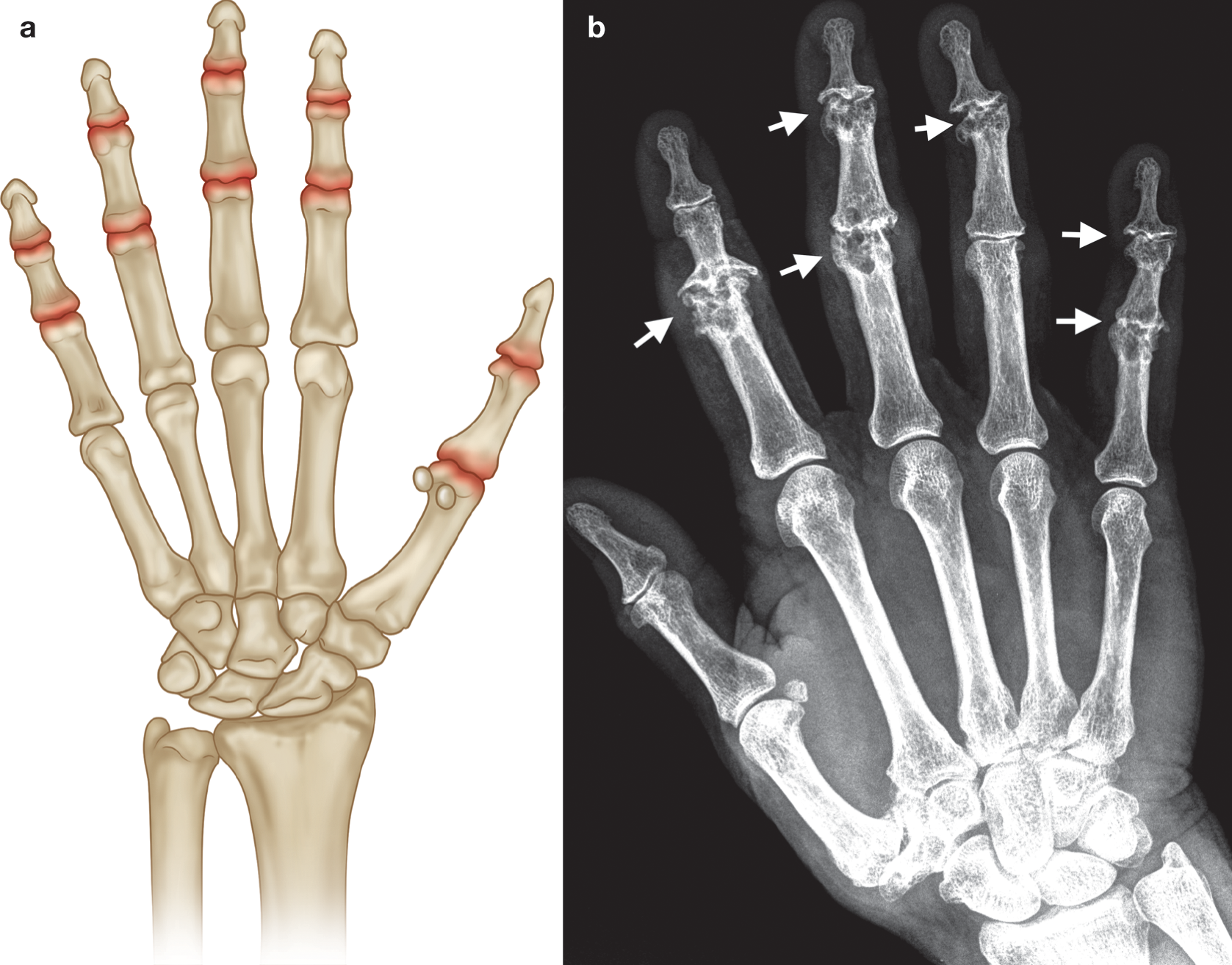
- Erosive osteoarthritis is a subset of primary OA and predominantly involves the hands.
- The PIP and DIP joints are more commonly involved although any of the above joints in primary OA may be involved.
- There are bony outgrowths at the joint margins, joint space loss, and central erosions. The latter produces the “seagull” appearance.
- The disease may progress with eventual ankylosis.
- The lack of marginal erosions, periosteal reaction, and new bone formation, other than osteophytes, helps to separate the disease from psoriatic arthropathy.
Erosive osteoarthritis
 info_outline
info_outline
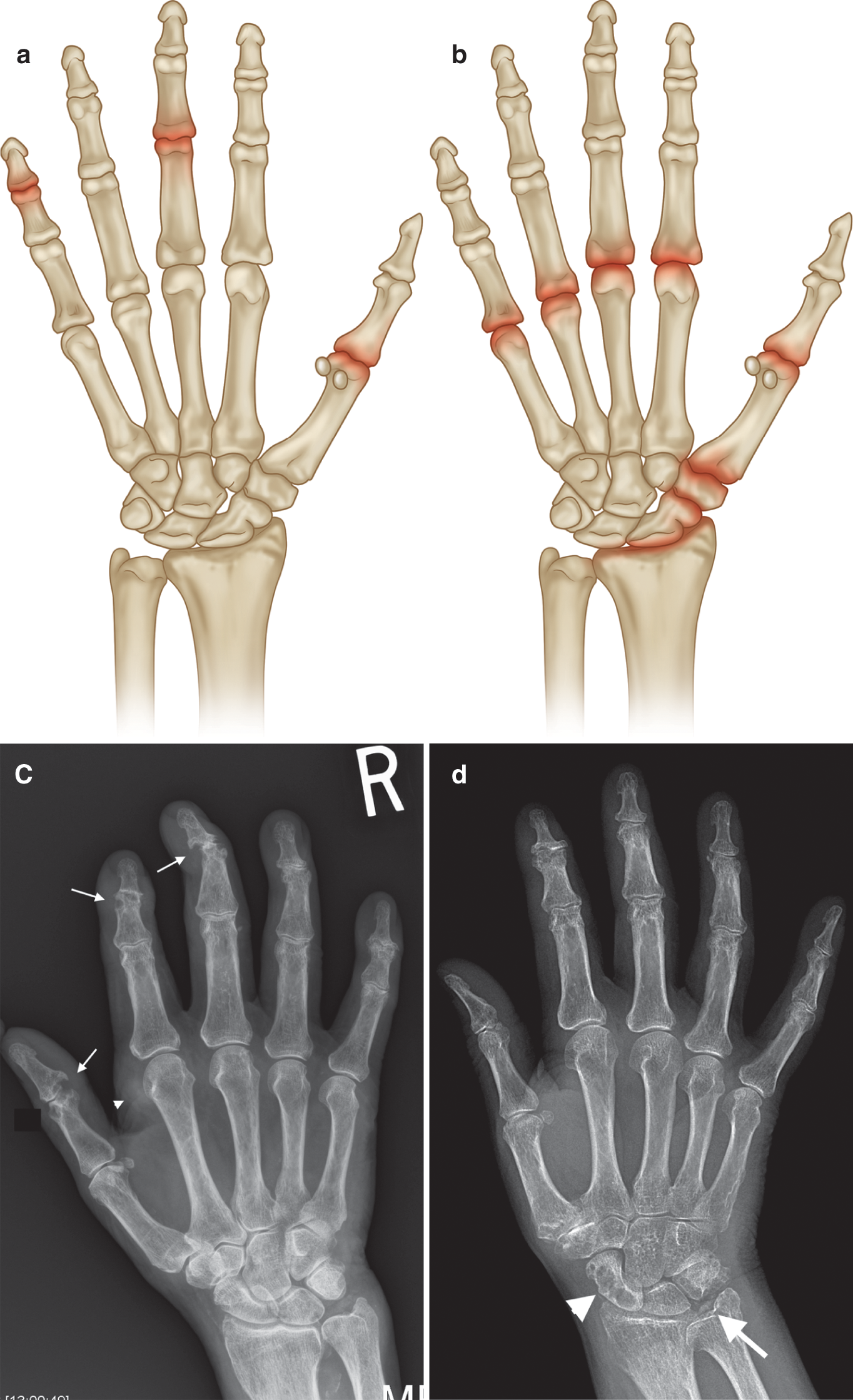
(a) Common sites of involvement with osteoarthritis of the hand (highlighted in red). (b) PA radiograph of right hand with early osteoarthritis demonstrating joint space loss at the PIP and DIP joints and early subchondral cysts at the second and third
 info_outline
info_outline
(a) Common sites of involvement with erosive osteoarthritis of the hand. (b) PA radiograph of right hand with changes of chronic erosive osteoarthritis at the PIP and DIP joints (arrows) with classic central erosions and “gull wing” osteophytes (most
Rheumatoid Arthritis
Hands
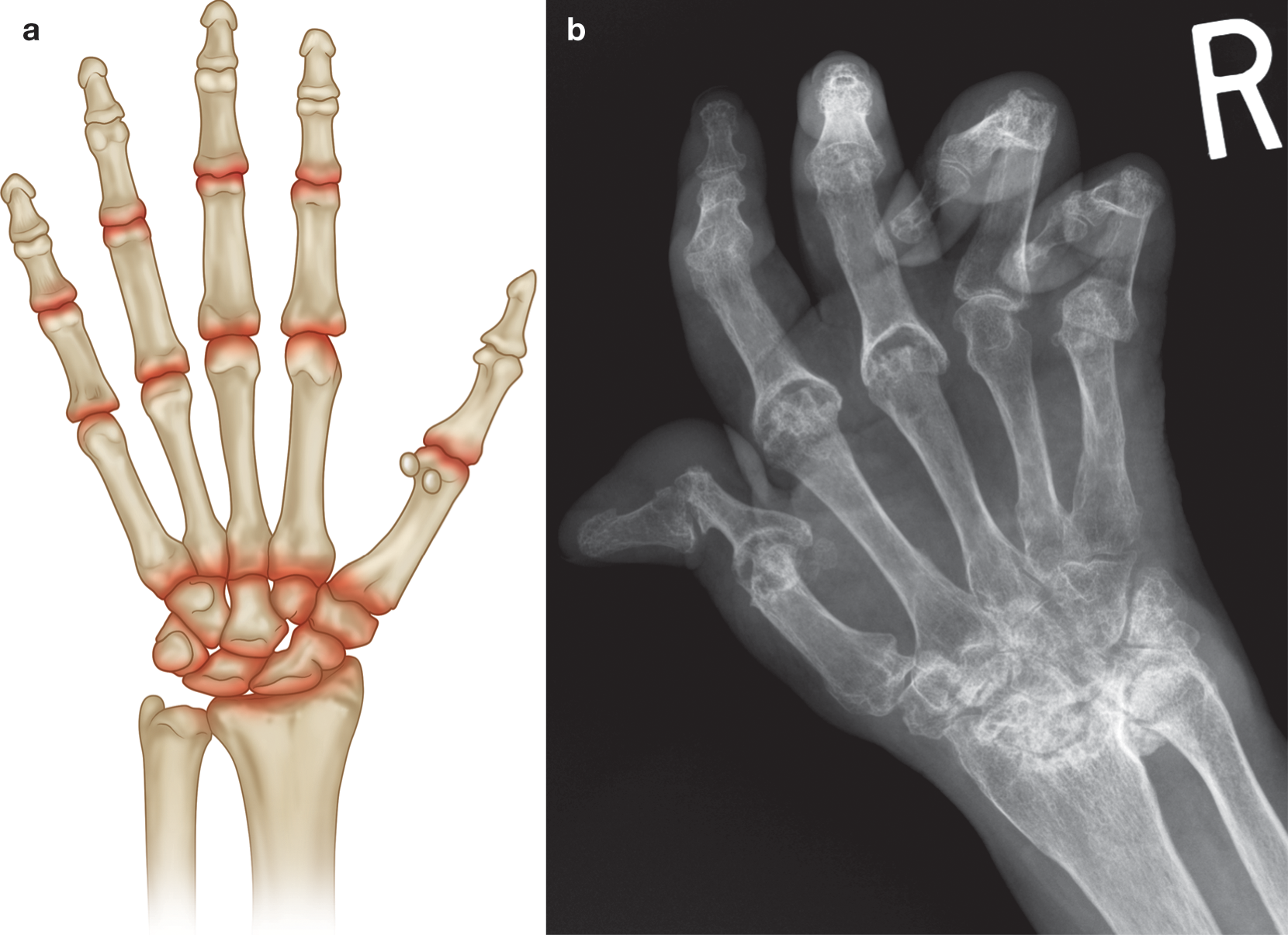
- Symmetrical involvement of the PIP, MCP, and wrist joints (symmetry is a key feature in that both hands are involved rather than perfect symmetry).
- Feet are also involved in RA with similar joints being involved, i.e. PIP and MTP joints. The fifth metatarsal head is a common first site of erosion.
Other Joints
- Elbows, glenohumeral, cervical spine, hips, knees, and ankles are the most common involved joints in RA.
- Note that lumbar spine is almost never involved. Again symmetry is typical but perfect symmetry is not absolute.
 info_outline
info_outline
(a) Common sites of involvement with rheuma- toid arthritis. (b) PA radiograph of right hand with changes of long-standing rheumatoid arthritis (similar changes were noted in the left hand and wrist in keeping with sym- metrical disease). Marked diffuse osteopenia, extensive erosions at radioulnar joint, partial collapse at proximal carpal row, erosions at the MCPJs and first IP joint, “Z” shaped deformity in the thumb, subluxation at the fifth MCPJ, and flexion deformities at the PIPJs
Seronegative Arthritis
(Ankylosing Spondylitis, Reactive Arthritis, Psoriatic Arthritis, Enteropathic Arthritis)
Hands
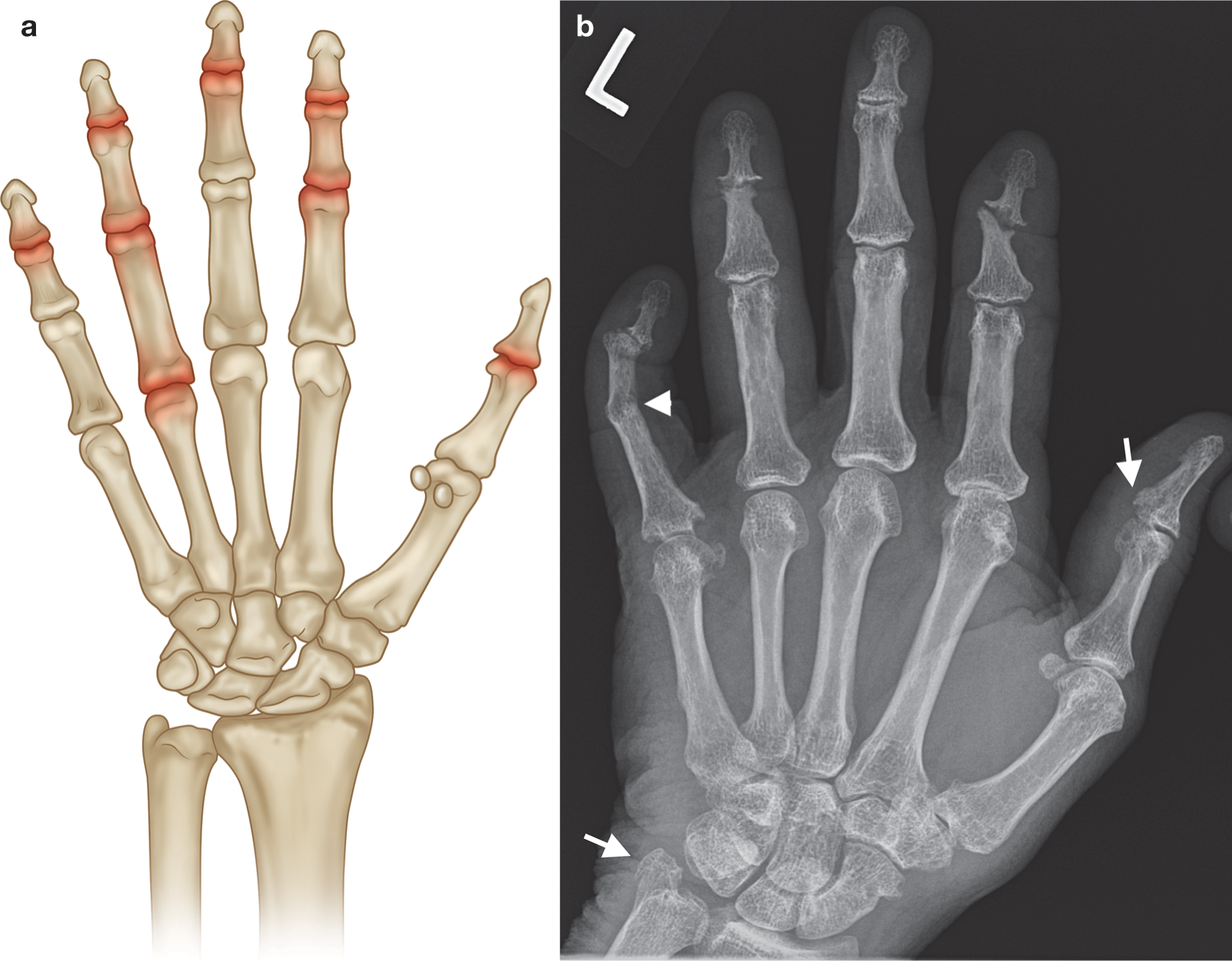
- Several patterns can be found in PsA, in particular the distal form (DIP involvement) and the symmetric polyarthritis pattern that can mimic RA (PIP, MCP, and wrist involvement).
- Periarticular osteopenia occurring in RA and periostitis (laying down of new bone) occurring in PsA are helpful in differentiating RA from PsA.
Other Joints
- All seronegative arthritides can affect the sacroiliac joints (SI).
- AS by definition involves the sacroiliac joints symmetrically, whereas the other types may affect SI joints asymmetrically
- Lumbar and thoracic spine are involved, but cervical spine is less commonly involved, with the exception of PsA
- Lower extremity asymmetric large joint oligoarthritis is classic and is found in the hip, knee, and ankle joints
 info_outline
info_outline
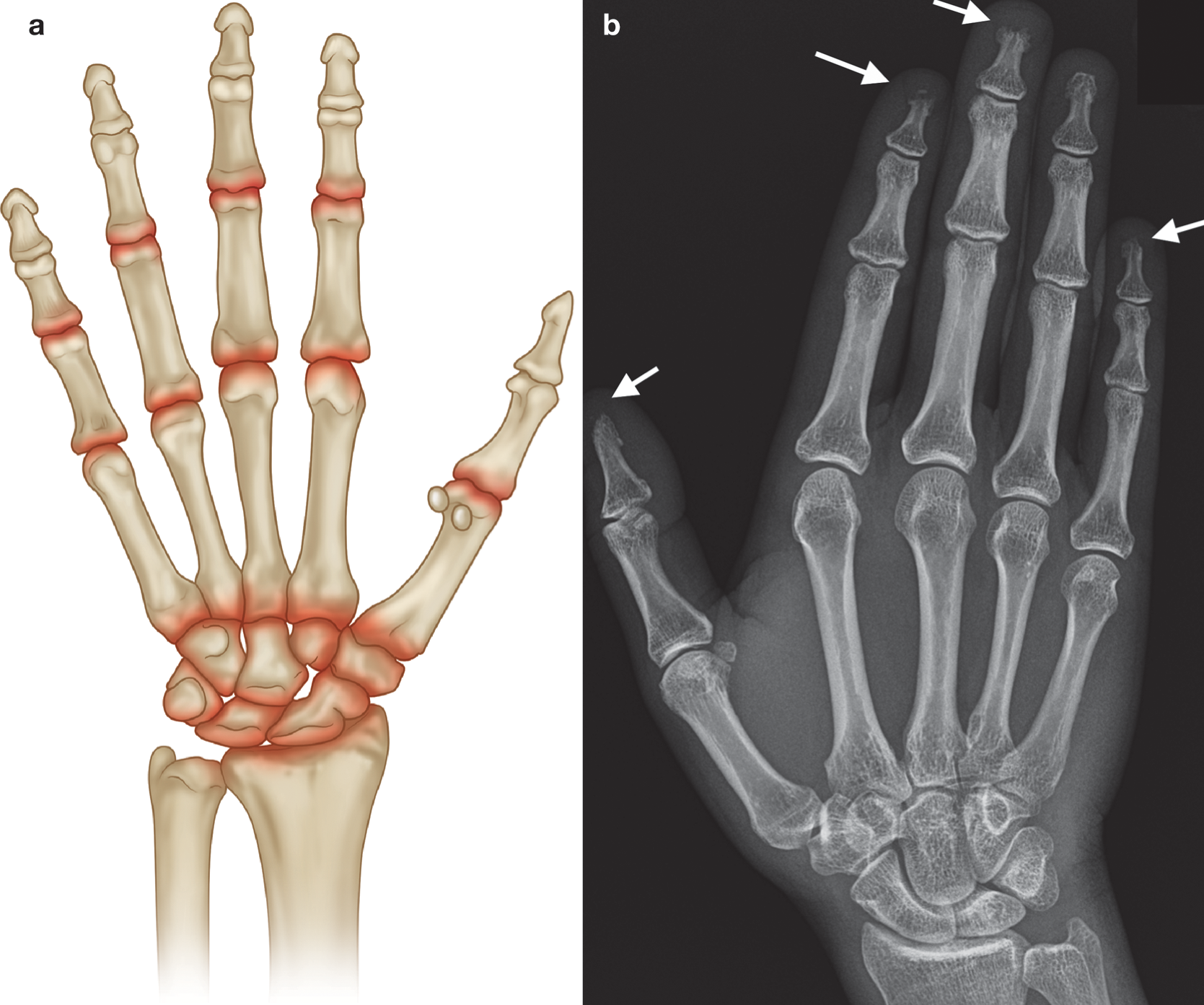
(a) Common sites of involvement with seronegative arthritis. (b) PA radiograph of the left hand in a patient with long-standing psoriatic arthritis (asymmetrical changes were present on the right hand). Normal bone density, new bone formation at ulnar styloid and base of the first distal phalanx (arrows), marginal erosions at the distal scaphoid and the fifth MCPJ and DIPJ, central and marginal erosions at the second and fourth DIPJs, and joint fusion at the fifth PIPJ ( arrowhead ). gouty tophus ( arrowhead). Note absence of periarticular osteopenia. There was asymmetrical left hand involvement (not shown). d ) PA radiograph of the right hand with chondrocalcinosis triangular fibrocartilage ( arrow ), normal bone density, mild joint space loss at the MCPJs, moderate degenerative changes at the first CMC, and crystal-related prominent subchondral cysts of the scaphoid. Incidental mild osteoarthritis, age-related, at the PIP and DIP joints in ( c ,d )
Crystalline Arthropathies
(Gout, CPPD)
Hands
- Any joints of the hands can be affected in gout or CPPD arthropathy.
- When these diseases become chronic and recurrent, they often mimic rheumatoid arthritis.
- In the case of CPPD, this clinical presentation is termed pseudo-rheumatoid arthritis.
- Plain radiographs would be of great help especially if it shows OA of the second and third MCPs as well as calcification in the cartilage of the triangular fibrocartilage complex (TFCC) of the wrist.
Other Joints
- Almost any other joints can be involved in crys- talline arthropathies, but involvement of the spine, except for atlantoaxial joint, is unusual
- The first MTP is classically the first joint to be involved in gout (podagra).
 info_outline
info_outline
Common sites of involvement with (a) gout and (b) CPPD arthropathy. (c) PA radiograph of the right hand in a patient with a 15-year history of gout and chronic renal failure with marginal erosions (arrows), some with overhanging edges (first IPJ), and
Connective Tissue Disorders
(SLE/ Scleroderma/Polymyositis/ Dermatomyositis/Sjogren’s)
Hands
- SLE often involves the hands in the typical RA distribution (PIPs, MCPs, and wrists) and can have the same deformities as RA (swan neck and boutonnière), but the lack of erosions on plain radiographs is a key differentiating factor in long-standing disease.
- The pattern of reversible joint deformity is termed Jaccoud arthropathy.
 info_outline
info_outline
(a) Common sites of involvement with connective tissue disease. (b) PA radiograph of the right hand with scleroderma demonstrating resorption at phalangeal tufts (arrows), acro-osteolysis. No significant overlying soft tissue atrophy or soft tissue calcification