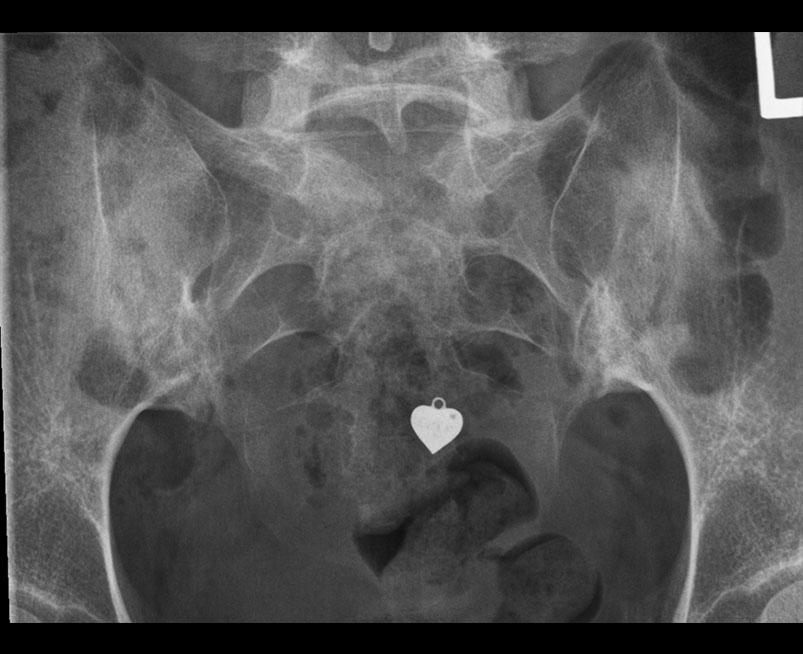
Modified New York Radiographic Grading
Grade |
Imaging Findings |
| Grade 0 | Normal |
| Grade 1 | Suspicious Change |
| Grade 2 | Minimal Abnormality-small localised areas with erosion or sclerosis without alteration in joint width |
| Grade 3 | Definite Abnormality- moderate or advanced disease including partial ankylosis |
| Grade 4 | Severe abnormality- total ankylosis |
 info_outline
info_outline
 info_outline
info_outline
 info_outline
info_outline
 info_outline
info_outline
 info_outline
info_outline